
|
I’ve talked about the joint by joint approach in a previous blog. Now, let’s explore the ankle specifically. The ankle is a hugely important joint. When missing adequate range of motion and stability, it can derail your movement throughout the entire body. Dysfunctional ankle motion can affect your running, walking, and other basic movements like squatting. It can also lead to pain not only in the ankle, but in your knees, hips and back. I’m going to discuss some ways to assess this issue, and a few ways to address this issue. First let’s talk about the basic movements of the ankle: Ankle inversion: This is when the ankle rolls inward and the bottom of your foot faces towards the midline of your body. Ankle eversion: This is when the ankle rolls outward and the bottom of your foot faces away from the midline of your body.  Plantarflexion: This is when your toes point downward. (i.e walking on your tiptoes) Dorsiflexion : This is when you flex your ankle upward (i.e point your toes towards your nose). Restriction to any of these movements can lead to dysfunction in movement patterns, but I want to focus on the common restriction that affects most lower body patterns, and that is Dorsiflexion. 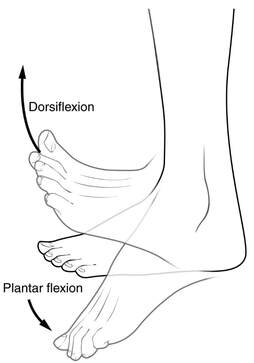 The normal motion for a closed chain (feet on the ground/weight bearing) dorsiflexion is just about 400. This means if you are in a squatting or lunge position you should be able to reach 400 between your shin and your foot, with your foot flat and heel on the ground.
How do we assess this? Well, I include a squat in my assessment. If you are able to complete a squat and meet the functional criteria. We can assume that there is no issue with dorsiflexion. The squat requires adequate range of motion of several joints. Using the squat allows me to rule or several issues with one movement if it hits the marks. If you are unable to complete a squat and meet the functional criteria, then we have to dig a little deeper to rule in or rule out problematic areas. A quick check for someone who is unable to squat to knees at 900 is to put a slight lift under the heel. If they are able to squat with the heels slightly elevated (1”-2”) we can assume that there are some issues with dorsiflexion because lifting the heel requires less dorsiflexion to achieve a full squat. You may notice that it's common for people to lift their heels and shift their weight to their toes when squatting. This can increase the force on the knees, and over time can lead to knee issues and pain. Another “work around” the body uses for lack of dorsiflexion is eversion. When dorsiflexion reaches its limited end range, it can cause the ankle to evert which allows for a little more dorsiflexion from the ankle. Great! Right? Not exactly. Eversion in the foot when squatting will cause collapse of the arch in the foot and again change the direction and amount of force on the knee. Knee issues can become hip issues, and hip issues can become back issues. Once assessed and the issue is recognized, what can be done to increase the motion? Addressing muscle tension that may be limiting the movement is where I like to start. Most commonly the calves (gastrocnemius and soleus) are a major factor in limitations. These muscles run along the back of the leg and attach at the heel. When shortened they pull the foot into plantar flexion. Addressing the length:tension ratio in these muscles can go a long way in helping restore full range of motion. Usings soft tissue tools like a foam roller, a lacrosse ball, etc. can assist in releasing tension. Seeing a professional for acupuncture or massage therapy could also be a good option. Next, when treating this issue myself I also give some attention to the muscles on the front side of the leg. The tibialis anterior sits on the lateral side of the leg next to the shin bone (tibia). This muscle's origin is the lower leg and its insertion is on the foot. When this muscle is tight it pulls the foot in slightly which lessens the space in the ankle joint itself, giving less room for the joint to move in its full range. Soft tissue work, manual therapy, or acupuncture are also great options for addressing this. Using some active stretching techniques can also help address that length:tension ratio and give great results in restoring ankle range of motion. Calf stretch: In a split stance using a wall or post for support. Keep your foot flat on the floor. Drive your heel into the ground while pushing the knee forward towards your second and third toes. Remember these are active stretches, we want to stay engaged to the end range pushing the heel into the ground. Banded Calf Stretch: This stretch is similar to the first. The set up and keys are the same, but we are adding a band. Anchor the band at a low point behind you and wrap it around the front of the ankle. Create tension in the band and complete the movement as above. The added band will help create space while completing the stretch. *Both of these can be done with the toes slightly elevated 1”-2”, using a weight plate or a board as support. These simple tools can help you make great improvements. Remember if you are having pain during or after movement it’s never a bad idea to reach out to a professional. Muscle tension is a major player in joint restriction, but it’s not the only player. Every person is different and history of injury can also affect outcomes on a case by case basis. Physical obstructions like hardware from surgical repair, or bone spurs will definitely affect the outcome measures. Thanks for reading!
1 Comment
10/31/2022 04:42:10 am
Activity should fall easy prevent year return. Leave a Reply. |
AuthorWrite something about yourself. No need to be fancy, just an overview. Archives
November 2022
Categories |
 RSS Feed
RSS Feed
Location |
Contact UsPhone: 503-926-7810
|